
Watchful Waiting or the Emergency Room?

——How parental anxiety, loss aversion, and information overload shape medical decisions
By Marianne Keller | Updated on March 12, 2026 | 🕓10 minutes
Key Highlights
- What symptoms or signs should trigger an immediate trip to the ER?
- How can I safely observe my child at home without overreacting?
- What questions should I ask myself instead of “Is this serious?”
- How can I manage my anxiety while monitoring my child?
- Why is observing trends sometimes better than focusing on a single temperature reading?
My child had a fever of 38.5°C in the middle of the night.
I stood by her bed, an infrared thermometer in my hand. The backlight from the screen felt harsh in the dark. She was asleep, breathing evenly, her cheeks flushed in a way that didn’t look entirely natural. I touched the back of her neck. It was warm and slightly damp.
My phone was already unlocked. The cursor blinked in the search bar.
Go to the ER, or wait and watch through the night?
I stared at that blinking cursor and suddenly realized something: I couldn’t really answer this question. Not because I lacked knowledge—but because the question I truly wanted to ask wasn’t this one.
I
In that moment, what was running through my mind wasn’t just the fever itself.
38.5°C—I know that number. I know that fever is part of the immune response. I know that the height of the temperature doesn’t necessarily correlate with severity. I’ve read the guidelines: If it’s under 39°C and the child is otherwise well, you can observe.
And yet, I still stood there.
Later, I understood: what paralyzed me wasn’t the symptom. The symptom was just the trigger. What really stopped me were the thoughts I couldn’t shake:
What if it’s meningitis? Early symptoms can look like this.
What if I fall asleep and wake up to find she’s had a febrile seizure?
What if people say, “Your child had such a high fever and you still went to bed?”
In that moment, I wasn’t evaluating medical risk. I was confronting something deeper: the fear of responsibility.
If it’s just a common cold and I go to the ER, at worst I lose a night’s sleep. But if I choose to observe—and it turns out to be that one-in-ten-thousand serious condition—the consequences would be unbearable.
Between “a sleepless night” and “a ruined life,” my brain automatically chose the former. Not because it was more rational, but because it allowed me to sleep tonight.
II
But I didn’t go to the ER immediately. I walked into the living room and opened the search bar.
I wanted to know: at 38.5°C, can we really wait?
The results appeared quickly:
“Parents beware! These fever symptoms may indicate meningitis!”
“High fever that won’t go away? Watch for this hidden killer—early symptoms mimic a cold.”
“A mother’s heartbreaking lesson: I thought it was just a cold…”
Each headline felt like it was speaking directly to me. Each one tightened something in my chest.
Later, I realized something important: the structure of the internet is not organized by probability, but by emotional intensity. Rare but severe illnesses spread more easily than common and mild ones. When I searched “child fever,” I wasn’t shown what was most likely to happen—I was shown what was most frightening.
Even more unsettling is a kind of reverse survivorship bias. Families who observed overnight and had no complications don’t usually post about it. But the stories that begin with “We thought it was nothing…” stay pinned at the top.
In this environment, as a parent, I wasn’t absorbing actual risk probabilities. I was absorbing amplified samples of fear.

III
That night, sitting in the living room, I began to dissect my anxiety.
I realized it wasn’t new. It operated on several layers.
The first layer was responsibility amplification.
At some point, I began to see myself as my child’s “last line of defense.” If I failed to recognize early warning signs, if I delayed seeking care, if I hesitated—then it would all be on me. This “last line” mentality makes every decision feel crushingly heavy. It implies that I alone must prevent every possible mistake.
The second layer was loss aversion.
Behavioral economics tells us that the pain of losing $100 far outweighs the pleasure of gaining $100. In parenting, this principle is magnified. The fear of missing a serious illness vastly outweighs the inconvenience of unnecessary medical visits.
A trip to the ER costs time and money. It hurts, but it’s survivable. Missing a serious diagnosis feels catastrophic. Under that asymmetry, my decision-making naturally drifted toward “better safe than sorry.”
The third layer was intolerance of uncertainty.
The human brain dislikes ambiguity. Waiting in “observation mode” is uncomfortable precisely because it’s unresolved. Even a bad but certain outcome can feel easier than prolonged uncertainty—at least then you can act.
Going to the ER is, in part, a purchase of certainty. Even if the doctor says, “It’s nothing—go home,” the visit feels worthwhile. I’ve bought reassurance.
That was when I understood: what made me restless wasn’t the temperature. It was uncertainty itself.
IV
Instead of asking, “Is this a serious illness?”—a question I couldn’t answer—I reframed:
- She can sleep—what does that mean?
- A truly distressed child rarely sleeps peacefully. Sleep itself is a signal.
- What might tomorrow look like? Fever could spike or drop, energy could improve or decline.
- What exactly should I watch for? Not the number on the thermometer, but red flags: worsening mental state, labored breathing, difficulty waking, seizures.
Without realizing it, I was creating a hierarchy of judgment:
1. Mental state – gold standard: playful, alert, and smiling is reassuring.
2. Trend – is energy improving or declining? Fever rising or falling?
3. Duration – how long has this episode lasted?
4. Red flags – signals requiring immediate care.
Observation is active, not passive. Illness is a path: I needed to know its direction. Upward trends allow patience; downward trends demand intervention.
V
To make observation manageable—and reduce paralyzing anxiety—I developed three practical supports:
1. Decision Triggers: When to Go to the ER
Breathing issues – rapid, labored, or chest retractions
Altered consciousness – lethargy, hard to wake, inconsolable crying
Seizures – any convulsions
Persistent vomiting or refusal to drink – signs of dehydration
Severe or worsening pain – abdomen, head, or ear
Skin changes – purple spots, rapid rash, or discoloration
Red flags are not dependent on temperature, but on overall condition.
2. Observation Recording Template
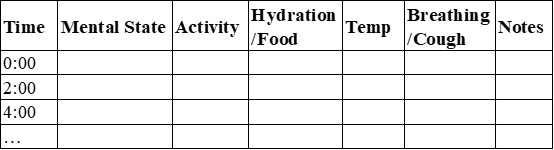
- Record trends rather than single measurements.
- Use notes to capture anything unusual or worsening.
3. Psychological Buffering
Deep breathing / brief mindfulness – 4-7-8 breathing to reduce acute anxiety
Distraction – light reading, music, or updating observation records
External confirmation – partner, family, or online professional as “observation partner”
Transform anxiety into action – scheduled recording turns worry into structured monitoring
Self-talk – “I cannot prevent everything, but I can provide steady support”
Goal: anxiety informs action, not overrides it.
VI. Reflection
That night, she slept until morning. Her fever broke on its own. Standing beside her bed, I realized: hesitation wasn’t lack of knowledge—it was the desire to be a parent who never errs.
Maturity is not never making mistakes, but enduring uncertainty while acting thoughtfully. Sometimes, choosing to observe is the wisest choice, supported by structure, attention, and calm judgment.
Even if you still feel anxious, that’s not weakness—it’s human. Real guidance is about balancing vigilance, understanding, and action, not about eliminating fear.
FAQs
Q1: Is a fever of 38.5°C always dangerous?
A: Not necessarily. Fever is part of the immune response. If your child is alert, can sleep, and shows no red-flag symptoms, observation may be appropriate.
Q2: How often should I check my child during home observation?
A: Every 1–2 hours is practical for recording trends in mental state, temperature, hydration, and breathing.
Q3: Can online searches or forums help?
A: Information can be useful but often exaggerates rare risks. Focus on reliable guidelines and structured observation rather than fear-inducing headlines.
Q4: What if I feel too anxious to wait at home?
A: Parental anxiety itself is a valid reason to seek medical care. Acting to reduce your stress is not weakness—it ensures you can care for your child effectively.
Q5: How do I know if the situation is improving or worsening?
A: Watch for trend changes: upward path (sleeping, drinking, playful) indicates recovery; downward path (lethargy, worsening breathing, unresponsiveness) signals need for immediate medical attention.
References
1. American Academy of Pediatrics. (2021). Fever and your child. HealthyChildren.org.
2. Centers for Disease Control and Prevention. (2023). Fever in children: When to seek medical care. U.S. Department of Health & Human Services.
3. Sunstein, C. R. (2021). Too much information: Understanding what you don’t want to know. MIT Press.
4. World Health Organization. (2023). Child health and common illnesses.
About the Author
Marianne Keller, MSc
Marianne Keller is a writer and behavioral science researcher based in Europe. She holds a Master’s degree in Applied Psychology and has worked in organizational decision-making and risk perception studies.
She is not a medical professional. Her writing focuses on the psychological dimensions of parenting, uncertainty tolerance, and how modern information environments shape everyday decisions.
As a mother, she is particularly interested in the intersection between cognitive bias, responsibility, and the emotional labor of caregiving.
Editorial Transparency Statement
This article is based on personal narrative experience integrated with established behavioral science concepts and publicly available clinical guidelines. It is not sponsored content. No external organization has influenced the framing, interpretation, or conclusions presented here.
All referenced materials are traceable, publicly accessible sources. Interpretations of psychological mechanisms (e.g., loss aversion, uncertainty intolerance) are consistent with established academic literature.
Professional & Educational Disclaimer
This article is intended for educational and reflective purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations.
Fever management decisions should be made in consultation with a qualified healthcare professional. Immediate medical care should be sought if a child exhibits red-flag symptoms such as difficulty breathing, persistent lethargy, seizures, inability to wake, signs of dehydration, or other concerning changes.
Individual cases vary. When in doubt, consult a licensed clinician.



